A Biased View of Dementia Fall Risk
The Facts About Dementia Fall Risk Revealed
Table of ContentsThe Facts About Dementia Fall Risk RevealedSome Known Incorrect Statements About Dementia Fall Risk Dementia Fall Risk for BeginnersThe Greatest Guide To Dementia Fall Risk
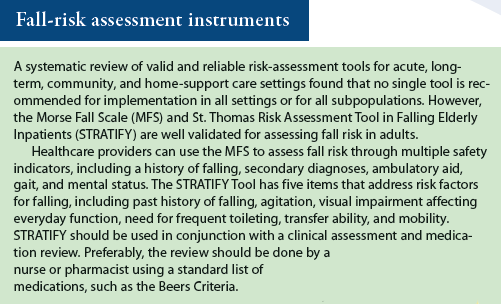
An autumn risk assessment checks to see just how likely it is that you will drop. The evaluation generally consists of: This consists of a series of inquiries regarding your overall health and wellness and if you have actually had previous drops or problems with balance, standing, and/or walking.Interventions are recommendations that may reduce your risk of dropping. STEADI includes three steps: you for your risk of falling for your risk variables that can be enhanced to try to prevent drops (for example, equilibrium troubles, impaired vision) to minimize your threat of falling by making use of effective techniques (for example, providing education and learning and resources), you may be asked several concerns including: Have you dropped in the past year? Are you stressed concerning dropping?
If it takes you 12 secs or even more, it may suggest you are at greater risk for an autumn. This test checks stamina and balance.
Move one foot midway forward, so the instep is touching the large toe of your other foot. Relocate one foot totally in front of the various other, so the toes are touching the heel of your other foot.
Dementia Fall Risk for Dummies
A lot of falls happen as a result of numerous contributing aspects; for that reason, managing the threat of dropping begins with determining the variables that add to drop danger - Dementia Fall Risk. Several of the most relevant danger aspects include: History of previous fallsChronic medical conditionsAcute illnessImpaired gait and balance, reduced extremity weaknessCognitive impairmentChanges in visionCertain risky medicines and polypharmacyEnvironmental elements can also increase the threat for drops, including: Insufficient lightingUneven or damaged flooringWet or unsafe floorsMissing or damaged handrails and get barsDamaged or incorrectly equipped equipment, such as beds, mobility devices, or walkersImproper usage of assistive devicesInadequate supervision of the people staying in the NF, including those who exhibit hostile behaviorsA effective loss risk management program calls for a comprehensive medical analysis, with input from all members of the interdisciplinary group
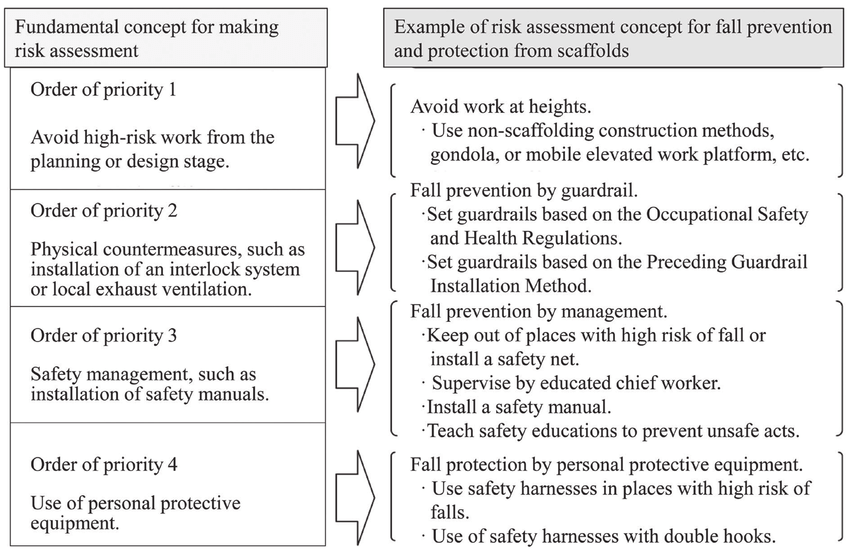
The care strategy should also include treatments that are system-based, such as those that promote a risk-free setting (appropriate lighting, hand rails, get click for source bars, etc). The efficiency of the interventions should be assessed occasionally, and the treatment strategy changed as essential to mirror modifications in the fall threat assessment. Carrying out a fall threat administration system using evidence-based ideal practice can minimize the occurrence of falls in the NF, while restricting the possibility for fall-related injuries.
Dementia Fall Risk for Beginners
The AGS/BGS guideline advises screening all grownups aged 65 years and older for autumn risk every year. This screening includes asking clients whether they have actually fallen 2 or more times in the past year or looked for clinical focus for a fall, or, if they have not dropped, whether they feel unstable when walking.
Individuals who have fallen as soon as without injury ought to have their balance and stride reviewed; those with stride or balance abnormalities ought to get added assessment. A background of 1 autumn without injury and without stride or balance problems does not necessitate further analysis past ongoing annual fall threat screening. Dementia Fall Risk. A fall risk assessment is needed as component of the Welcome to Medicare examination
Dementia Fall Risk Things To Know Before You Get This
Recording a drops history is one of the quality indicators for autumn prevention and monitoring. copyright medicines in particular are independent predictors of drops.
Postural hypotension can frequently be eased by lowering the dosage of blood pressurelowering medicines and/or stopping drugs that have orthostatic hypotension as a side effect. Usage of above-the-knee support pipe and copulating the head of the bed elevated might also lower postural reductions in high blood pressure. The suggested elements of a fall-focused physical evaluation are shown in Box 1.

A Pull time higher than or equivalent to 12 secs suggests high loss threat. Being not able to stand up from a chair of knee elevation without using one's arms shows raised loss risk.